British Columbia Mental Health Services
Historical Perspective to 1961
by: Richard G. Foulkes, B.A., M.D.
Click on the chapter headings, below:
The Asylum 1872-1901
Moral treatment
Custodial care 1912 to 1950
Renaissance
Summary
During the colonial period of the history of British Columbia, the only facility available for the mentally ill was the common gaol. John Robson, then editor of the British Columbian, later Provincial Secretary and Premier of the Province, described their custody in the New Westminster Gaol on July 23rd, 1863, "The cells in which they (the lunactics/R.G.F.) are confined are not at all adapted for such a purpose, entirely too small, ill ventilated, unheated and an offensive effluvia arising from beneath them, the result of no proper system of drainage".
In older colony of Vancouver Island, conditions were no less foul in the Victoria "lock-up", where Dr. J. S. Helmcken, B.C.'s first physician, saw the colony's earliest mental patients as far back as the early 1850's.
The facilities of Napay Asylum in San Francisco were also used occasionally, particularly for the committal of those insane members of the horde that traveled from this centre to Victoria en route to the gold fields of the Cariboo in 1358 and 1859.
Return to Index
THE ASYLUM 1872–1901
When female patients began to present themselves, the gaol became even more unsuitable so, that after an abortive attempt to house "lunatics" of this sex in a private home on Pandora Avenue in Victoria, the first asylum was established.
This was a "modest building" constructed of wood, 50 by 40 feet, that contained a number of "cells" or small single rooms. It was formerly the Royal Hospital, a pest house, and was located on the Songhees Indian Reserve in Victoria Harbour adjacent to the Marine Hospital. It accepted its first patient, a young woman referred by Dr. Helmcken, on; the 12th of October, 1872, just 14 months after B.C.'s entry into confederation. At the end of this first day of operation, the asylum was occupied by seven patients, all transferred from the "lock-up".
To look after these were an equal number of staff, including a Dr. Powell, the Medical Superintendent, and Mrs. Flora Ross, Matron. An "Insane asylum act" was promulgated the following year, 1873.
Within the next five years, in spite of the addition of a small wing, the facilities became inadequate and a second asylum, built at the cost of $24,000 was constructed as a replacement at New Westminster
on the present site of Woodlands School. This new Unit with a population of some 37 patients was opened in 1878.
The first annual report was not published until the year 1882. This document shows that the resident population had climbed to 49 and that the Institution was under a lay Superintendent, Mr. James Phillips with a Medical Officer, R. I. Bently, M.B., B.S.
The first New Westminster Asylum is described as an ugly building with windows so high that the outside could only be seen by standing on a table. Further, it was poorly heated by means of open grates and so overcrowded that two patients were compelled to share a single room. The following year some improvements were made to the buildings and, in 1885, the asylum was, once more, headed by a physician, Dr. Bently.
Mr. Phillips, henceforth, held the position of Steward. This year was, in addition, the first in which patients were allowed to work and the therapeutic effect on at least one of them is noted by Dr. Bently in the large, heavy, leather-bound case book that was the means of recording case histories in that day. We gather that improvement in a male patient discharged "cured" on the 12th of March, 1335, "...dated from the time '' he commenced to go out steadily to work every day" .
During this early period that continued to the enforced retirement of Dr. Bently in 1895 as a result of a Royal Commission inquiry the previous year, custodial care only was all that could be provided with a minimum of recreation and outside work. The only physician, embattled with the problem of keeping the per diem cost at a low level (it was 48¼¢ per day in 1891), of urging construction to house the increasing patient population, of ensuring adequate water supplies, and of visiting the Royal Columbian Hospital sometimes twice in a day in addition to writing his own letters, had little time for experiment, therapy or supervision.
The cruelty of the “Keepers” during this period was scandalous. As was stated in the report of the Royal Commission, composed of Drs. Hasel and Newcombe of Victoria, methods were in use that had been discarded in Great Britain more than a generation before. Equipment such as handcuffs leather mitts, pinion straps, camisoles, and straight jackets, with the cruel rope halter called "The Martingale" that could be used as a strangulation device, were in almost daily use. Also applied were tortures such as the "dip", in which a patient, arms handcuffed behind his back, was plunged head-down into a tub of cold water until he very nearly drowned and the "cage", a box constructed of wooden slats and made only large enough for a human body in which a patient might be kept confined for many hours.
In 1895, Dr. Boddington assumed the senior position. The attendants, who had implicated the grizzly affairs of the last regime, were forced to resign.
During the next few years, Dr. Boddington addressed himself to the task of humanizing the institution adding pictures to the walls, urging landscaping of the grounds, and reducing physical restraint. In addition he improved the food, constructed a much needed operating room, badgered the government of the day for increased maintenance funds, and started on a policy of the deportation of aliens who made up 70% of population in residence. On one occasion, he personally escorted to England a party of twenty-two “half-witted ne-ar-do-wells”, the progeny of wealthy British families who had been sent to the colonies as punishment for their failure to adjust to their parent country. Upon his return, he began formulating plans for the return of the Chinese, a large alien group that had given concern for many years.
In 1897, the Provincial Asylum was renamed the Public Hospital for the insane (P.H.I.) and a new act was promulgated incorporating within it an "Urgency Order" that had long been required.
In 1901, a Royal Commission, composed of Dr. C. K. Clarke, Medical Superintendent of the Rockwood Asylum, Kingston, Ontario, inquired into the operation of the institution. In spite of containing praise of the
Minimal restraint, good food, and the excellence of the new Surgical ward, Dr. Clarke's report criticized .the "excess staff" and the high wages that they were paid and recommended stricter economy, better bookkeeping (the old register was still the only record of the patient and slates were in use for passing messages from one nursing shift to another), further brightening of the wards, improved facilities for outdoor exercise, the establishment of a School for Nurses, and a Colony Farm as it was apparent that to bring about the required changes would entail an increased amount of work, Dr. Boddington “felt constrained through the advance of his years to relinquish the labour to younger hands”
Return to Index
Moral Treatment 1902 - 1912
These hands belonged to Dr. 0. H. Manchester who stated with optimism in the 1902 annual report that the Institution ".has entered upon a new century under new management, and moreover, has emerged from comparative insignificance and obscurity to become the largest.institution under the care and support of the Province of British Columbia.
The annual report, for the first time, contained a table of diagnosis. (Mania, melancholia, dementia and paranoia). Until this issue, the patient had been described but rarely labeled. Noteworthy is the fact that General Paresis formed 12% of the total number of admissions for the year (14 patients out of a total of 115). In addition, an "open-door ward" was reported and a statement of treatment principles was given that officially opened the era of ''Moral Treatment". These principles were listed as 1) essential medicines, 2) good food (there was a shortage that each patient, for example, being allowed only one egg per year and that at Easter), 3) regularity of living habits, 4) employment, 5) amusement, and 6) recreation.
A need for separate facilities to deal with acute cases, the mental defective, the tuberculosis patient, and the “criminally insane", was recognized and a need for musical therapy and industrial training was discerned.
During his first year in office, 1904, Dr. Manchester wrote into the annual report, the Kraepelin system of nomenclature. He announced, also that the Government had purchased 1,000 acres of land about twelve miles distant from P.H.I. near the junction of the Coquitlam and Fraser Rivers for purposes of expanding the mental hospital facility.
With C.E.Doherty, M.D.,C.M., Dr.Manchester’s successor, and Henry Esson Young, Provincial Secretary, the hospital for the Insane at New Westminster saw the full development of the principles of the “moral treatment of insanity”.
In addition to being the first year of Dr. Doherty's long tenure, 1905 marked the beginning of clearing of land for Colony Farm. Patients were segregated into "incurable", "curable", "feeble", and "infirm" upon admission. Rest, work, and amusement "judiciously selected" were basic treatment and a Musical Director was appointed, a Mr. Darcey, who organized an orchestra of institution employees.
Work was departmentalized and the "hospital" atmosphere:, heightened by using the word "nurses" rather than "keepers" or "attendants", and an attitude of kindness towards the patient was enforced by dismissal, if necessary.
With regard to therapy, none were denied exercise and fresh air, “patients”, Doherty wrote, “...walks the grounds by the hundreds". Medical treatment - work of all kinds in the shop or on the farm, and recreation -
was individualized and had the effect that Doherty, in 1907, could make the claim that the mechanical restraints of all kinds had been abolished.
After the introduction of hydro-therapy techniques to calm the few disturbed patients who remained, he added that "chemical restraint", also, was no longer in use.
The contemporary method of recording case histories was established and all physicians' notes were typewritten from 1908. The same year a Laboratory was established, with its work done by Mr. E.P. Hughes, a competent Bacteriologist, and, for the first time, research was added to the function of the institution. Detailed post-mortem examinations were carried out on all for whom permission could be obtained, investigations in the Spirochaetal etiology of General Paresis were pursued and thousands of observations of blood and urine were recorded and correlated with the mental diagnosis.
By the end of 1912, in spite of serious overcrowding, there was reason for optimism. Crops raised on Colony Farm exceeded the most sanguine expectations and the "farmer's Advocate" of December, 1912, describe it as "...the best equipped barns, stables, dairy equipment, and yards in Canada, if not the Continent". Dr. Doherty read papers before the B. C. Medical Society and the 68th Annual Meeting of the American Medical Psychological Association at Atlantic City, propounding his views of the treatment of mental illness for which he received approbation from many sources.
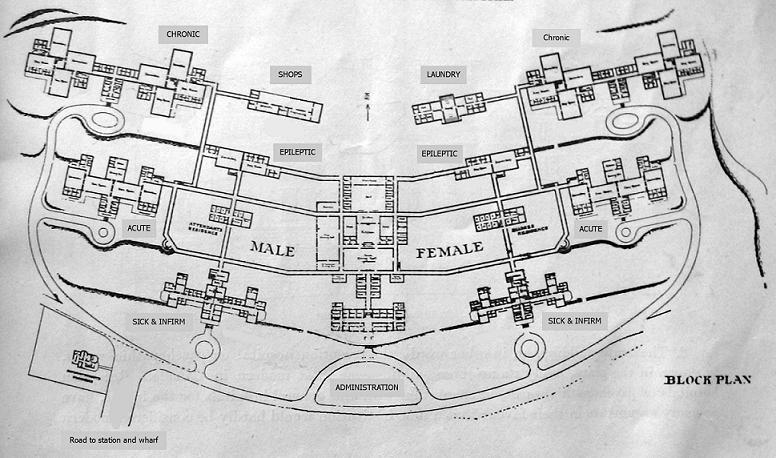
The plans for the new hospital at Coquitlam, obtained by staging a competition between the architects of the Province, received the highest commendation of psychiatrists in Eastern Canada and the Lunatic Commission of New York State. The called the building, in stages of a number of structures, each specialized as to function: and administration building, and acute building, sick and infirm buildings, an epileptic building, a pair of chronic buildings, and adequate living quarters for nurses.
It was decided that one of the chronic buildings should be constructed first so that it could be used to house the overflow from the P H I and the building now known as West Lawn was begun. The first building on the new grounds, named Essondale after Dr. Henry Esson Young The Provincial Secretary, was opened on April,1st 1913.
Two institutes were now in existence: the P.H.I. at New Westminster with Drs. J.S.McKay, and H. S.Steeves, and Essondale with Dr. Freeze as Assistant Medical Superintendent. Dr.Doherty was Medical Superintendent of each.
During the 1914 – 1918 World War, the dual institutions began to have increasing difficulties. Many of the nursing staff and Dr. Doherty himself left to join the armed forces. Mr. Hughes, upon whom the function of the laboratory defended, died late in 1913 and could not be replaced for 14 months.
During Doherty's absence, the annual reports were edited by Dr.J.S.McKay who, continuing in the same vein as his superior, pressed for buildings at Essondale, the new building already being overcrowded, and advocated the reporting of known cases of Syphilis now known to be the cause of 12% of admissions. He also requested training for the 43 mental defectives then in residence and amendment of the "Mental Hospitals Act”, to cover voluntary admissions.
In 1919, a six year old prison at Saanich on Vancouver Island was taken over to house the “criminally insane”. The same year, Dr.J.S.McKay resigned and started the Hollywood Sanatorium in New Westminster (70 beds) the only fully recognized private treatment centre for mental disease that the Province was to see until psychiatric wards were established at the Vancouver General Hospital (40 beds), and the Royal Jubilee Hospital in Victoria (24 beds).
Dr. Doherty died on August 14th, 1920. An era had passed and it would be thirty years before the same feeling of optimism would again pervade the institutions.
Return to Index
Return to custodial care 1912 – 1950
Dr. Doherty was succeeded by Dr. H.D. Steeves, who died on December 7th, 1926, and was succeeded in turn by Dr. A, L. Crease who continued as head of the organization until March 31st, 1950.
During the 38 year period between the opening of the first building at Essondale and the resurgence of activity highlighted by the establishment of the Crease Clinic of Psychological Medicine, progress was slow and sporadic and regression in some aspects of patient care took place.
Each of the buildings added during this interval, before they were officially opened, were doomed to become the site of suffocating overcrowding at an estimated average of more than 55% of rated capacity.
The resident population at the end of each ten year period during this interval increased by approximately one thousand. In 1912, it was 722, in 1924, when the first "acute building" now known as Centre Lawn was opened it had risen to 1,784; in 1930 when East Lawn was opened for women, 2,411.
By 1951, the number resident at the end of the year was 4,602.
During this period, wards overflowed into the attics and basements, choking out areas needed for day use and therapy, especially for that of the occupational and recreational variety. On the wards, conditions were such that, towards the end of the period, there were more patients than beds. Those unfortunate enough to be in excess had to sleep on mattresses placed on the floor. Furthermore, a return to locked wards and even to physical restraint took place.
As many as 30 patients in restraint and 51 in seclusion, mostly women, were counted by an inspection team as late as 1951.
Efforts to provide well trained professional staff during this period moved forward when, in 1925 a Miss Van Wyck, a registered nurse, became "Superintendent of Nurses" and the first with this qualification to hold this important executive position. An "Instructress of Nurses", a Miss K. Mallott, was appointed in 1930 and the first Nurses Training School was established. June, 1932, saw the first graduation exercises addressed, appropriately, by Dr. H. Esson Young, then Provincial Health Officer. The first male graduates did not appear until 1940 and then were only five in number.
The Nursing Services, built up by 1938 to an. enviable ratio of two registered nurses to one psychiatric nurse and one student, were devastated by war. The sudden resignation of forty-one trained (most of the R.N.’s) and seventy-two partially trained staff in 1942, reversed this ratio and resulted in the hiring of aides “…of various standards”. There was at this point 56.5% new staff devoid of any experience in hospital work or psychiatric training.
A change in hiring policy, in 1944, brought married women, mostly psychiatric nurses, back to the staff and relieved the situation. By 1945, male training, stopped in 1940, was resumed and, by 1947, the nursing problem had been stabilized but with a new ratio of 18 registered nurses, 44 psychiatric graduates, and 192 nurses-in-training.
The solution to the problem of providing separate facilities for the acute mental-patient, the mentally defective, and the tuberculosis had to await the 1950 period but some changes were made that ameliorated conditions and assisted in "setting the stage".
With regard to the mentally defective, an effort, inadequate from the outset, to establish a school was made at Essondale in 1920. Dr. Steeves, in 1922, was the first to suggest using the P.H.I, for this purpose. This suggestion was underlined by the Royal Commission of 1925 that dealt in great detail with mental deficiency and sounded the keynote for the future that the problem was "...educational rather than medical" The number of mental defectives increased through the years. In 1927 they numbered 200; by 1930, 400. The transfer to P.H.I started in 1932 and was near completion with five school teachers on staff when the "Schools for Mental Defectives Act" came into being in 1953.
Similar temporary measures were affected with the tuberculosis patients. The first attempt at isolation in 1938 was unsuccessful as these patients were placed on wards with patients suffering from other illnesses.
In 1940, two separate wards one for each sex, were formed and were soon crowded with a total of 300 cases, 200 of whom were classified “active”.
Facilities for the care of the acute mentally ill remained inadequate because of overcrowding, although a psychopathic ward was established in the Centre Lawn building in I924, with facilities that were improved when compared to those that had existed for so many years. The Royal Commission of 1925 recommended the conduction of a separate institution a "psychopathic hospital", as was in existence in the eastern United States, but this was not to come into being until the Crease Clinic of Psychological Medicine with its 300 beds, was constructed in 1948 by adding a wing to the recently vacated Veteran's Building built 13 years before.
Special provisions for the aged psychotic became available in 1936 when the buildings of the Boys' Industrial School, abandoned in favor of the Borstal system and located on property adjacent to Essondale, were utilized as "Homes for the Aged". This collection of two story buildings, architecturally resembling Tudor style, and constructed on the side of a large hill were obviously unsuitable for elderly patients but, nevertheless, fulfilled a need.
Various departments were formed during this period that, although each suffered from severe limitations, were available when resurgence occurred. Directors were found for Occupational Therapy and Recreational Therapy. Physicians on staff were appointed to direct or to work in major departments such as, Pathology, X-ray, and Pharmacy but held these positions as duties secondary to their ward work, so that activity in one field was detrimental to effort in the other. A study of the reports on the laboratory, for example, reveals a variable load, usually contingent on the presence or absence of a laboratory technician, as well as the freedom of the Medical Officer in charge. A successful attempt was made to keep up with the admission serology tests and the routine examinations of water and food, but routine blood and urine examinations fluctuated as did the number of autopsies performed. The chief cause of death for many years is given in the reports as "exhaustion, due to.." followed by the psychiatric diagnosis. This diagnosis was most frequent in years such as 1931 when only one autopsy was performed on 304 deaths and least in years like 1937, when 51 autopsies were carried out on 236 deaths.
A social service department was established in 1932 with the appointment of Miss J.Killburn, R.N., a trained social worker. This action was based on a recommendation made by Dr.Steeves in 1926.
This constantly understaffed group carried a large work load that was composed of case work done not only for the Mental Hospitals but also for the Child Guidance Clinic established in Vancouver on July 15, 1932 and later expanded to include Victoria, (1934) and the traveling clinics to Nanaimo and Chilliwack (1935).
The department also administered psychometric tests to various groups, including the Borstal Home candidates, and accepted responsibilities to lecture to classes at U.B.C. All members of this department were responsible to the Welfare Branch until 1957 when they were transferred to the Department of the Provincial Secretary.
A psychologist, Mr. Watson, M.A., was appointed in 1937, thereby relieving the social work department of much of the labour expended in administering psychometric tests.
There were definite advances in treatment during this period but limitations of staff and space reduced the number of patients to whom many of these could give benefit. By 1926, intravenous tryparansamide had been used for Syphilis and found to be effective but palliative only for General Paresis. During this year, malarial therapy was begun and, by 1933, G.P.I, showed, a definite decrease in frequency. By 1946, with bismuth, sulfa, and penicillin added to the therapeutic agents, treatment definitive. The purely physical treatments were less dramatic but gave rise to much optimism. Hydrotherapy, the chief physical treatment in the 1907 period, continued in use to the 1950's. The use of insulin shock was first reported being carried out on 20 patients at a time, in the 1938 report. At this time, metrazol therapy introduced but was not too promising from the beginning. In 1940, to give an idea of the number affected, there were 239 patients on insulin shock and 301 on metrazol that is, 540 patients under treatment out of a total population of 3836.
Insulin treatment was decreasing during the war years owing to the lack of trained staff. At the same time, electroconvulsive therapy came into use and replaced the dangerous and much hated metrazol. Surgery for mental illness was introduced in 1946 when 9 lobotomies were performed in the Vancouver General Hospital by Dr.F.Turnbull. The following year, there were 45 cases and over the next five years, psycho-surgery suffered a gradual loss of popularity as other means of therapy became available.
Return to Index
Renaissance 1950
March 31st, 1950 was the 1ast day of the 35 year career in the P.M.H.C. of Dr. A.L. Crease. It also marked the beginning of a new phase in the treatment of mental illness in the province. By this date, in addition to the Departments of Pathology, Pharmacy, Social Work, Psychology, Occupational Therapy, and Recreational Therapy that had been formed over the previous three decades and was now in charge of specialists, there was added a Department of Neurology. In addition, there came into being a new facility for the aged at Vernon, “The New Vista” a rehabilitation centre for discharged female patients, and the Crease Clinic, dedicated to the intensive treatment and rehabilitation of the acutely ill and to education and research.
When Dr._A.M. Gee, Dr. Crease’s successor, accepted on April 1st, 1950, the senior position in the Mental Health Services, the population, in residence was 4,602. On this date, the various mental health activities were amalgamated into the Provincial Mental Health Services. Divisions were formed, governed by a "Hospital Council". These divisions were called
1) The Active Treatment Services,
2) Geriatrics Division,
3) Preventive Services,
4) Rehabilitation Services,
5) Research Division.
At the same time, the New Westminster Mental Hospital was re-named Woodlands School in keeping with its function, although direct admission would not tike place until 1953, the word "attendant" was deleted from the Civil Service Structure, and the Provincial Mental Hospital's "Chronic Buildings" were renamed "Lawn Buildings", thus updating the semantics of mental illness. Pennington Hall, containing a cafe, bowling alley and theatre, was started as were increased facilities for the aged at Terrace and for the patients at Woodlands School. The Nursing School at this time had centralized its training heretofore carried out independently by both mental hospitals, and commenced a "block system" for its 230 female and 190 male students. In addition, the annual report for this year, 1950, carried the nomenclature of the American Psychiatric Association, thus spelling an end to the system that had been used for many decades.
In 1950, the Medical Faculty of the University of British Columbia started to train its first class of undergraduates. The high hopes were expressed in the annual report for the year that the new school would be of great assistance with the vexing problem of post graduate training for resident physicians of the mental health services, who were, by this time, severely restricted by regulation formulated by the Royal College of Physicians and Surgeons. They could, for example receive credit for one year only towards certification regardless of the number of years spent in the mental hospital, and further, were to be encouraged to train in several centres rather than remain in the same geographical area. By 1961, a firmly organized, integrated scheme was yet to be developed, although co-operation in many fields, particularly neurological research, had continued.
On January 1st, 1951, “The Clinics of Psychological Medicine Act” was proclaimed and “…for the first time it became possible to receive patients at an earlier stage of their illness” This moment, long sought caused plans for a second large hospital to be shelved and stimulated thought on the next advance - the reaching further into the community with day hospitals and out-patient clinics. This latest “Act” made voluntary admissions and certified admissions without the loss of civil rights possible for a maximum period of four months.
The first year of operation of the Crease Clinic was indicative of success. 791 of the 963 patients admitted were returned to the community within the statutory period. During this year (1951-1952), the first consultants in general surgery and neuro-surgery were retained by means of a "Mental Health Grant" and a survey of overcrowding was made at the request of the Federal Government. The results of the latter shocking, one building (the male side of Centre lawn) was found to be 81.1% overcrowded; that is, a facility designed for 143 patients housing 260. West Lawn (male), East Lawn (female), and Centre Lawn (female side) were 30.8%, 56.8%, and 42.5% overcrowded respectively.
The year, 1951 marked the commencement of a policy to establish "open wards" in the P.M.H. and Crease Clinic. The following year, all forms of physical restraint were, once again, abolished, except for seclusion under strict safeguards and, a year later, children under six years of age were permitted direct admission to the Woodlands School, thereby ending the tragic mixing of small patients with adults suffering from various types and degrees of mental disorder.
During 1951, a research "colony" was established at the University under Dr. W. Gibson and investigations were begun. 1952 saw the opening of operating room facilities in the Crease Clinic. Since the peak days at the Public Hospital for the Insane, all surgical operations, at great inconvenience to all, had to be carried out either at the Royal Columbian Hospital in New Westminster or the Vancouver General Hospital. This year a remotivation program for long neglected patients in the “chronic” buildings was started in the female building, and in harmony with this increased activity, regular ward rounds were commenced and two social workers were appointed to begin full time work on two wards in the Provincial Mental Hospital (P.M.H.). Alcoholics, long refused admission for treatment; were allocated 25 beds in the Centre Lawn Building.
In 1953, a “School for Mental Defectives Act" became operative on the 1st of October. Woodlands School at this time had 1,098 patients “on the books” and a growing waiting list. On the wards of both the P.M.H. and the Crease Clinic, the "relationship" or "mileau therapy" was incorporated into the teaching program and the team approach of physician, nurse, psychologist, and social worker was stressed. Insulin Coma, which had been discontinued at the P.M.H., was re-introduced and marked the point at which treatments available in the Clinic were also in use in the P.H.H. Group psychotherapy, including an adolescent group, was practiced volunteer workers, organized by the Canadian Mental Health Association (C.M.H.A.) appeared for the first time on the wards, and out-patients services were established for discharged patients to be used, especially, by those who resided in the nearby geographic area.
Oh April 1st, 1954, the Neurological Research Centre which had published an impressive list of titles and whose members had presented papers to numerous societies, was formally transferred to the University to become the Department of Neurological Research.
By March 31st, 1955, there were five unlocked wards in the P.M.E., and the Crease Clinic, serving 537 patients, definite progress was being made. General Paresis, the scourge of so many years, was practically eliminated. Epilepsy was under control, and it was calculated that 50% at least of schizophrenics could be assisted back to the community after a relatively short period of treatment. Chlorpromazine and Reserpine were added to the armamentarium.
By this time, too, the community's involvement in the treatment of mental illness was obvious and it had such representatives as the. CM.H.A. volunteers and the Auxiliary formed at Woodlands School by, the B C. Society for Handicapped Children. The personnel of the Provincial Mental Health Services participated in many community-sponsored efforts in the field. They assisted in the Mental Health Training Program that was held under the direction of the Vancouver School Board, in addition to advising the Alcoholism Foundation of B.C., and the Narcotic Addiction Foundation.
On May 4th, 1955, a centre for the treatment of tuberculosis, the North Lawn building containing 230 beds, was opened after many years of anticipation. On January 2nd, 1957, the “Mental Health Centre" in nearby Burnaby was opened. This unit provided accommodation for the Child Guidance Clinic which was freed from its long residence in antiquated, inadequate quarters and was to provide out-patient services and a day care centre for the community. The same year, the quarters vacated by the Child Guidance Clinic were converted into "Venture", a rehabilitation centre for men.
Dr. Gee retired on August 31st, 1953 and his position as Director was taken by Dr. A.E. Davidson. The next year the Mental Health Services were removed from the Provincial Secretary's Department where they had been since 1872 and were transferred to the Department of Health Services and Hospital Insurance. Dr. Davidson became a Deputy Minister representing the P.M.H.S. and moved his office from Essondale to Vancouver.
During the 1959 - 1960 fiscal year, considerable expansion took place in the areas dealing with the aged and the mentally defective: an infirmary building named the Valleyview Building at the Homes for the Aged, Port Coquitlam, was opened; and 130 males were transported from Woodlands school to Tranquille, a recently vacated sanitarium at Kamloops, no longer required for the treatment of large numbers or Tuberculosis cases.
At Essondale, approximately 70% of the patients were living on open wards and the result of 10 years of increased therapy were now available for comparison and were cause for exultation. In 1948- 1949, the total population increased by 354 with an index increase of 28.09. In 1959-1960, the increase was 20 with an index of 0.61%. The total admissions in 1943-1949 were 1,260. In, 1959-1960, 3,294. For the first time in history, there were actual decreases in the resident population; 78 patients less in 1956-1957, and 90 less in 1958-1959.
Return to Index
Summary
It may be added, in summarizing, that the history of the treatment of mental illness in the Province of British Columbia is, to the largest extent, the history of the development of the Provincial Mental Health Services.
This extends now from 1872 to 1961. Starting as an institution to provide custodial care chiefly for the dependant insane, it developed prior to the first World War into a model demonstrating the principles of the “Moral treatment" of mental illness that were in vogue in that day. This was followed by a long time interval, marked at each end by a devastating war and plagued throughout by episodes of economic depression. During this there was a slowing down of construction and a consequent building up of and overcrowding problem in addition to a periodic shortage of trained personnel that not only reduced the efficiency of the organization as a treatment centre but re-introduced, some at least, of the restraining practices of a previous barbaric time. During this period, however, sporadic but important advances were made that were available for development during the resurgent period of the last decade.
During the resurgent period, there have been some definite advances as shown by statistics (and when scrutinizing these we must keep in mind the sobering facts that there is a long waiting list for Woodlands School and for the Homes for the Aged and that many of the persons discharged from the long term buildings in the P.M.H. remain public charges in boarding and nursing homes). There has, in addition, been a re-establishment of the "Hospital" atmosphere with wards made as cheerful as is consistent with continued overcrowding. Facilities for occupational therapy, recreational therapy and amusement have been improved as have the means for providing treatment - Psychiatric, Medical, and Surgical - to those patients to whom these can bring benefit. Finally, there are encouraging signs of rising community interest in mental illness and commencing expansion of the mental health services to provide facilities within the community itself to all who can be accommodated with no regard for socio-economic status.
Return to Index






















{kind=link}